
A new drug is making headlines around the world for being the first ever to slow the progression of Alzheimer’s disease.
After an 18-month trial of 1,800 patients, lecanemab slowed patients’ mental decline by 27%.
Although scientists are hailing a “new era” in treatment, strains on the NHS and the scale and complexity of the disease mean it could be a long time before patients and their families can really get the benefits in the UK.
What is Alzheimer’s – and how is it different to dementia?
Alzheimer’s disease is the most common form of dementia.
Dementia is the umbrella term for a group of conditions that cause the brain to decline and result in memory loss, confusion and difficulties carrying out daily tasks.
Other types of dementia include vascular, mixed dementia, dementia with Lewy bodies, and frontotemporal.
Alzheimer’s causes proteins to build up in the brain and form abnormal structures sometimes called ‘plaques’ or ‘tangles’, which kill off nerve cells and brain tissue.
It also makes it harder for chemical signals to be sent between brain cells.
Symptoms
All forms of dementia are gradual and get worse over time.
The trajectory of the disease is different for each patient and some will decline quicker than others.
Generally it is split into three stages – early or mild, moderate or middle, and severe or advanced.
Symptoms of Alzheimer’s disease include:
- Memory loss
- Reduced mental sharpness
- Difficulty remembering words or trouble speaking
- Problems with movement, including eating, drinking and walking
- Changes in behaviour or personality
- Low mood
Alzheimer’s is life-limiting in two ways.
Studies have shown it can be closely linked to other physical health conditions such as cardiovascular disease and diabetes.
But in the later stages of dementia a person’s immune system is weakened and they are likely to be unable to swallow or go to the toilet independently.
This increases the risk of infection and other conditions that can result in death.
Life expectancy depends on when a person is diagnosed – but is roughly eight to 10 years, which is longer than the other forms of dementia.
How common is it?
More than 850,000 people in the UK have dementia but this is predicted to exceed one million by 2025 as more people live longer.
The majority of them – 520,000 – have Alzheimer’s.
One in 14 people over the age of 65 have dementia, which increases to one in six people in the over-80s.
According to the most recent Dementia UK report in 2014, it costs the UK £26.3 billion a year – more than cancer, heart disease and strokes.
Although the NHS pays £4.3bn of that – the social care sector pays more – £10.3bn.
This is because most dementia is managed in the community and care homes – not in hospitals.
Hospitals are often only involved in diagnosing the condition and caring for patients who are admitted with other or related medical issues.
Two-thirds of the total £26bn annual cost is paid by patients, their families and carers.
According to Dementia UK’s director of clinical services Paul Edwards: “The NHS is already struggling to provide care for the growing number of people living with dementia, in part due to the absence of post-diagnostic and community support.”
His charity is calling on the government to honour the promise it made in May to produce a 10-year dementia strategy.
Are treatments available now?
Unlike some other types of dementia, people with mild or moderate Alzheimer’s are offered medication.
People in the early or moderate stage of the condition can take either donepezil, rivastigmine or galantamine, which all work by boosting chemical messengers in the brain.
They may also help reduce anxiety, which is often experienced by dementia patients as their cognition declines.
Those with moderate or severe Alzheimer’s may be offered a drug called memantine, which also boosts chemical messengers but can also reduce challenging behavioural changes and delusions.
There is no cure for dementia, so all drug treatments currently available will only work for a limited period of time and do not slow the progression of the disease, just the symptoms.

New drug to target Alzheimer’s
Why is lecanemab different?
As Dr Susan Kohlaas, director of research at Alzheimer’s Research UK, explains: “This is the first time a drug has been shown to both reduce the disease in the brain and slow memory decline in clinical trials.
“Although the benefits were small and came with significant side effects, it marks the arrival of a treatment that can slow the course of Alzheimer’s disease.”
So while current treatments only reduce symptoms, lecanemab can reduce amyloid proteins in patients’ brains, which kill off nerve cells and tissue.
In practical terms, the study suggests that over the course of 18 months the drug delayed patients’ worsening of the disease by five months.
This could be built on by other drug companies and trials to give patients, their carers and loved ones more time with a better quality of life and fewer symptoms.
Will it be available on the NHS?
There are big barriers to lecanemab being available on the NHS.
This is because it only works for people in the early stages of Alzheimer’s and current pressures on the health service mean that one in six people wait more than a year to see a specialist after being referred by their GP.
By that stage – it would be too late for most patients to benefit.
And because the drug works by reducing amyloid proteins, they have to be detectable on a brain scan before it can be prescribed.
According to the Alzheimer’s Society one in 10 people wait more than six months for a brain scan, again reducing the window lecanemab can be used.
Read more:
Govt ‘should provide dementia care insurance’
70,000 living with early onset dementia
Symptoms can start two years before diagnosis
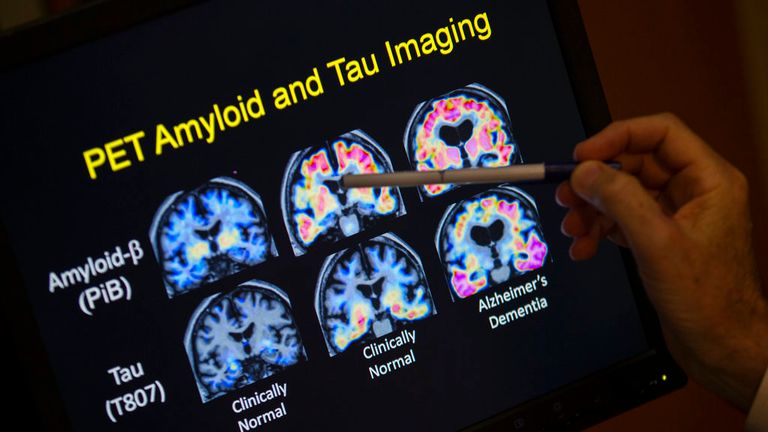
The brain scans used by the NHS to help diagnose dementia are also often MRI or CAT scans.
They only eliminate other possible conditions like tumours – or show brain shrinkage and changes to blood vessels – not the build-up of proteins.
A small percentage of patients are then sent for PET scans, which do show amyloid proteins – but they are not widely available.
Thirdly, many dementia patients get diagnosed with ‘unspecified dementia’ – 6.6% of over-65s and 17.2% of under-65s in 2021.
This means they can’t be offered lecanemab because it only works for Alzheimer’s specifically.
What needs to be done?
Dementia charities and research bodies say increasing NHS access to PET scans and blood testing that can also help with Alzheimer’s diagnoses is key.
Dr Richard Oakley, associate director of research at the Alzheimer’s Society, says: “This highlights more than ever the need to prioritise early diagnosis, through wider access to PET brain scans and research to get blood tests into the clinic, so people can access these drugs when they become available.”
His colleague Fiona Carragher, director of research and influencing, also stresses the importance of early diagnosis in general.
“We could feasibly see a situation where people sit on waiting lists for so long that their disease progresses too much to receive what could have been a life-changing drug,” she says.
“We urgently need to focus on better ways to diagnose people quickly and accurately while they’re in the early stages.”